
Introduction
A recent study carried out in Italy has emphasized some meaningful data: almost one fifth (1/5) of patients suffering from chronic pain received no treatment while hospitalized (1); besides, 25% of the patients who referred to centers for pain management reported that the intensity of their pain had never been assessed (2).
In 2010 the national legislature passed a new law [Legislation decree n. 38, in line with the Declaration of Montreal (3)] intended to better manage the pain in patients, as well as to limit the diffusion of this complex phenomenon which strongly affects the Italian national health service. According to Article n. 2 of the Law, pain therapy is referred to as “….all the diagnostic and therapeutic actions carried out on patients suffering from chronic pain by employing any pharmacological, instrumental or psychological therapy, as well as any rehabilitation or surgical intervention, in order to outline specific diagnostic and therapeutic strategies to better manage and control pain…..” (4).
This regulation is favorably welcomed by other European and non-European; however, it is disappointing to admit that three years after entering in force, this law has not showed the expected outcomes as its application is still ongoing. Although in Italy, as well as in many other countries, pain management assessment has never been enforced by specific laws, access to treatment has strongly improved in these last years and this has guaranteed efficient therapies and pain management approaches in line with the scientific international guidelines.
Considerations on the inadequate management of pain: what happens in Italy
Several are the considerations for tackling why pain management strategies are inadequately applied (6).
– Lack of awareness: you have to keep in mind that any change implies a certain degree of resistance. It is therefore important to endorse a new way of thinking in order to improve the level of awareness and overcome the resistance itself (7).
– Emerging problems related to health institutions: multidisciplinary approaches are nonexistent, pain management is not given the right priority, nurses have a limited amount of time they can dedicate to pain assessment, as they are often interrupted by several other activities. Cittadinanzattiva, which is a consumers protection association, has carried out a survey on a national scale, where it emerged how difficult it is to have access to treatment, and how the median waiting time to access a center for pain management varies from months to years (9).
– Patient related problems: in many societies, cultures and religions pain is believed to be a natural part of one’s own life and health status. Italy is a country where many different cultures intermingle, and it is mainly among senior citizens that there is still the belief that not much can be done to relieve pain (10). Pain assessment and management should mainly be carried out by health personnel in general, although the patient’s will has to be taken into account. All information regarding the potential management of pain should be shared with the patient so that the therapeutic intervention may be tailored on his/her needs and bring some relief. Indeed, the patient’s decisions have to be respected and it is fundamental to provide all the information in a clear and satisfactory manner; as well, the various possibilities of therapeutic intervention have to be clearly outlined as well. In particular, chronic pain does have important implications on the spiritual sphere, as well as on the general physical welfare: it makes the patient reflect on the meaning of life and his sense of being left alone and abandoned by God, thus experiencing a social isolation.
It is therefore important to support and protect the citizen from misleading low-quality online information, not at all corroborated by scientific studies (11). It is still common for a patient to be strongly influenced by friends and relatives on the best therapeutic interventions to follow.
An Italian survey focused on the accessibility to pain centers highlighted an important data: it seems that the percentage of patients who refer to these centers are advised by word of mouth to do so by friend and relatives (38%), while only 18% of them are recommended to turn to specialized facilities by their general practitioner (12). We would like to point out that, to date, many citizens from ethnic or racial minorities still experience a disparity of treatment in accessing health care services. The discrimination is usually determined by several factors:
- stereotypes,
- clinical information,
- decision making plans,
- income (13),
- mental disorders,
- gender (discrimination against women),
- drug history,
- linguistic barriers,
- little awareness on health issues,
- patients affected by specific painful pathologies,
- comorbidity (14).
– Emerging problems for healthcare personnel: inadequate knowledge and limited possibilities in pain assessment and management: the reluctance to use opioids, their possible side effects and potential addiction/tolerance (opiophobia) are issues which need to be kept in mind. Only a few years ago, in Italy therapies based on opioids were almost lacking and this inevitably caused negative drawbacks on clinical practice. Thanks to Legislative decree 38/2010, the use of opioids in Italy has become simpler. The WHO, which takes the per capita consumption of morphine a relevant National Health Service indicator, has clearly classified Italy as having one of the worst standards in the EU (15). Thanks to the continuous updating of health personnel in improving their level of expertise, as well as the innovative academic curricula addressed to new professional health figures, it is now possible to overcome inefficient and outdated cultural stereotypes and open up to a new approach to pain management.- Therefore, effective pain management is not only a comprehensive and ongoing task affecting the health service, but it an essential indicator of civilization of any country and shows what its health care system may offer (16).
Pain management and accredited nursing training in Italy
As stated by the International Association for the Study of Pain (IASP), pain is a multidimensional and complex phenomenon that requires an efficient approach and effective management based on actual knowledge. The nature of pain is multidimensional and as such it has to be approached (17). The definition of “pain” used by IASP (1986) and by the WHO is broad and generic, therefore no healthcare professional can exclusively manage such a phenomenon in an autonomous way. This would be impossible. Nurses must be aware of their central role and responsibility and must be knowledgeable about their profession and ready to serve as advocates for the person in pain. An adequate training and a continuous update will allow health personnel to achieve the necessary level of expertise in pain assessment and management.As the Italian Ministry of Health said (18) and as condemned by Cittadinanzattiva (consumers protection association) (19), “…the issue of pain is very often limited to marginal studies in university education, both in degree students or post-degree fellows; as well, training programmes do not pay sufficient attention to this important subject matter”. In the Italian Faculties of Medicine, which include medical, nursing, physiotherapy and healthcare staff courses, pain management classes are started up and implemented only if the Dean of Faculty or the teaching staff agree to do so; besides, optional courses do not always satisfy the needs of the future medical personnel or other healthcare professionals. In Italy specific Specialization courses on pain assessment and management exist but there is no specific training for pain specialists”. An Italian research carried out an investigation to determine the post-bachelor training possibilities in 41 Faculties of Medicine and 15 Faculties of Psychology in the academic year 2010-2011 (before the implementation of Legislative decree 38/2010): the evidence is overwhelming and reported in Map 1.

The results highlighted an heterogeneous distribution of pain management courses throughout the territory, and it also showed how the training was mainly offered to medical or nursing staff, excluding other healthcare professionals. These courses were basic (also addressed to nurses) and advanced (only for doctors), offering a high standard training (20). Apparently, the problem does not affect Italy alone – it has also been analyzed by the Association of American Medical College (21) – and this has to be taken as an encouragement to train highly qualified staff by finally updating university curricula and post-doctoral courses.
Among the many objectives, pain management training needs to focus on how to improve the patients quality of life (22). A recent Italian survey (23) investigated the general level of knowledge of students, and brought to light the inadequate preparation on how to assess and manage pain with pharmacological and reliable approaches. Only 0.5% of the students had attended training courses in pain management facilities and 37% of them had trained in pain management while attending Nursing, Oncology, Bioethics and General Medicine courses. These latter had been organized by teachers who were attentive/sensitive to this issue, although there was no real definition of how the training curricula were structured and organized. It is interesting to underline that the nursing teaching staff, even if not academically structured, was the most sensitive to the issues of pain management and relief.
For the academic year 2012-13 Italian universities have created training programs in line with the decrees implementing Law 38/2010. They are first degree of master, often in combination with palliative care issue. The Master, in accordance with the directions of the Decree of 4 April 2012, (Establishment of the Master’s degree in “Palliative care and pain management for health professions (12A04293) (OJ No. 89 of 16 April 2012), providing health care professionals a non-medical training highly qualified also in the treatment of pain.
Training objectives
Specific training on pain management will have to be multidisciplinary and interprofessional and involve healthcare professionals. The level of competence and experience of the person who cares for a patient suffering from chronic pain is strongly related to his professional evolution and training updates (24). This implies the need for highly specialized and multi task professionals able to deal with relational and educational issues and management skills specifically needed to care for chronic pain patients. Highly qualified professionals must be able to outline a treatment schedule to relief, reduce or manage pain to allow patients to quickly get back to their lives, possibly eliminating or reducing drug dependency and use. Absolutely mandatory in Italy is the need to give higher credit to highly specialized nursing assistance, and this may be achieved only by re-viewing and standardizing the present curricula and by guaranteeing different levels of training, basic and advanced. This latter may be achieved only if the degree in nursing will finally be structured to provide a deeper and more complete competence in advanced clinical practice, considering that at present nursing studies are mostly oriented to research and administration management issues. However, thanks to Legislative decree 38/2010 (25) advanced clinical practice skills can be achieved by the 1st level master course on “Palliative care and pain management”, which confers a recognized academic title and allows the professional nurse to operate in public health facilities, as well as in non-profit Institutions especially designated for palliative care and pain management. This master is set up by the Faculties of Medicine with an experience in pain management and palliative care. This course is structured and based on a multidisciplinary approach, which includes theory lessons, training experiences and individual study sessions. The final exam consists in discussing the thesis and takes into account the overall judgment of the teaching staff and/or tutor.
The objectives of the master course, for nurses / pediatric nurses can be summarized as follows:
I) current knowledge of the physio-pathology and of the evolutionary chronic diseases in chronic pain patients;
II) knowledge of the diagnostic and therapeutic approaches to assess physical, psychological, social and spiritual needs;
III) knowledge of the psychosocial skills aimed at the activation of internal and external resources to the patient and his family;
IV) knowledge of the treat chronic pain and ability to recognize the symptoms of advanced late onset illnesses;
V) knowledge of the psychological and spiritual aspects which affect a patient experiencing chronic pain at the end of his life, the use of specific tools for assessment of acute and chronic pain and quality of life;
VI) ethical and legal problems related to palliative care and pain management, communication and interpersonal skills aimed at effective communication with the patient, family and team, to respect for their dignity and the will of the patient, ability to handle ethical issues related to end of life and chronic pain;
VII) Competences of the clinical skills designed to identify and verify the significance of the rehabilitation / occupational diseases in the patient with a chronic evolution and in the patient with chronic pain (26).
Recipients and access requirements
The Master’s degree is reserved for health workers in possession of Bachelor of Nursing in the health area, Pediatric Nursing, Physiotherapy and Occupational Therapy or equivalent bachelors (26).
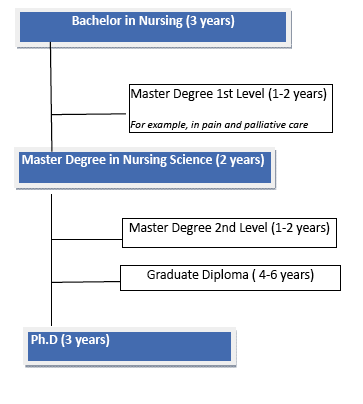
Italian Universities have never activated specialization courses (post degree courses) addressed to nurses; however, a good alternative could be offered by PhD programmes. Figure 1 summarizes the nursing academic training in Italy.
Some countries have implemented doctoral courses (Doctor of Nursing Practice), which are specifically aimed at training nursing staff in advanced practice, paying special attention to the translational techniques used in clinical practice, thus forming multi task clinical experts (27). This will allow to train highly qualified staff for the assessment and management of pain, in line with the healthcare strategies active in other countries.
The most pressing problem to be solved is to clearly define the boundary between nursing and medical competence, a limit which has been overcome in other countries, which is still rather confused in Italy. Although nursing training is carried out in academic institutions, to date the professional skill achieved through a qualified training of this kind is not officially recognized (Legislative decree 739/94). Indeed, an improved professional level of expertise has to correspond to a greater professional autonomy, to a greater efficacy and to a greater visibility within the country. This highly qualified staff must be able to face healthcare problems in a more timely and efficient way. There is no clear differentiation in the level of competence between nurses with a Bachelor degree and those with an MA degree or a master.
A high profile professional training should therefore lead the academic teaching staff to orient the curricula towards the achievement of a higher level of expertise, not only in clinical practice and healthcare management, but also to improve one’s own communication skills so that understanding and taking care of the person in pain may finally be seen as a multidisciplinary approach (28).
Conclusions
Today, although Italian nurses, are not responsible for the prescription of pain medicine, the decision making to manage pain medication, monitoring the effects, after demand of patient, is a responsibility of the nurses. In Italy, the course of studies in pain management starts from a basic level of a three-year (bachelor Degree) academic course and can be followed by a master training course. Legislative decree 38/10 addressed to all non-medical healthcare professionals is only oriented to 1st level masters for trainings on pain assessment and management. Unlike what happens on the international scenario, in Italy higher levels of education (Master degree, Residency, Doctoral Research) do not contemplate a specific clinical training for those employed in pain management activities. This gap has to be bridged in the shortest time possible in order to be in line with the European provisions and, above all, to guarantee timely and efficient interventions to satisfy the complex needs of the population, affected by painful oncologic and benign diseases.
Education provides us with the tools and expertise to better deal with pain management issues; however, keep in mind that education is and must always be supported by years of experience and clinical practice (29).
References
1. Sodo S, Cartoni C, Cerbo R, Lo Russi S, Reale C, La Torre G. Prevalence of pain in the hospital: results from a survey among inpatients in a teaching hospital. Ig Sanità Pubbl 2012;68(3):421-34.
2. Latina R, De Marinis MG, Cattaruzza MS, Sansoni J, Gatti A, Di Biagio E, Camilloni A, Notaro P, Guzzetti V, D’Angelo D, Mastroianni C, Casale G, Tarsitani G, AND Pain Clinic Group Characteristics of the adult population who attend centres of pain clinic in Italy. Posters Session. Pain in Europe. 8th EFIC Congress – European Pain Federation of IASP Chapters, Florence, Italy 9-12 October 2013.
3. International Pain Summit. Declaration that Access to Pain Management is a Fundamental Human Right. IASP: 2011.
4. Disposizioni per garantire l’accesso alle cure palliative e alla terapia del dolore. Legge 15 Marzo 2010, n. 38.
5. Sodo S, Cartoni C, Cerbo R, Lo Russi S, Reale C, La Torre G. Prevalence of pain in the hospital: results from a survey among inpatients in a teaching hospital. Ig Sanità Pubbl 2012;68(3):421-34.
6. The Joint Commission International. Approaches to pain management. An essential guide for clinical leaders. Second Edition, Oakbrook Terrace, Illinois (USA): 2010.
7. International Association for the Study of Pain. Guide in pain management in low-resource setting. IASP Press, Seattle: 2010.
8. Rejeh N, et al. Ethical challenges in pain management post-surgery. Nurs Ethics 2009;16:161-172.
9. Cittadinanzattiva Onlus. Non siamo nati per soffrire. Dolore cronico e percorsi assistenziali. Tribunale per i Diritti dell’ammalato. 2009.
10. Shea M, McDonald DD. Factors associated with increasing pain comunication in older adults. Western Journal of Nursing Research 2011;32:196-206.
11. Kaicker J, Debono VB, Dang W, Buckley N, Thabane L. Assessment of the quality and variability of health information on chronic pain websites using the DISCERN instrument. Bio Medical Center Medicine 2010;8:59.
12. Latina R, Sansoni J, De Marinis MG, Cattaruzza MS, Mastroianni C, Casale G, Notaro P, De Angelis F, Guzzetti V, Camilloni A, Tarsitani G and PCG (Pain Centers Group: Adducci E, Carassiti M, De Meo MA, Proietti R). Accessibility to the treatment of chronic benign pain. Survey into Italian pain clinics. ICNP, Melbourne, Australia. May 2013.
13. Smedley B, Stith A, Nelson A. unequal treatment: confronting racial and ethnic disparities in health care. Washington, DC: National Academic Press; 2003.
14. Green CR, Anderson KO, Baker TA, Campbell LC, Decker S, Fillingim, Todd KH, Vallerand AH. The unequal burden of pain: confronting racial and ethnic disparities in pain. Pain Med, 2003; 4(3): 277-294.
15. Conferenza Stato Regioni e Ministero della Salute, Approccio globale al dolore cronico, iniziativa nell’ambito della giornata del sollievo. 2002.
16. Felicetti V, Gareri R, Capomolla E, Cristina G, Cifaldi L, Terapia del dolore: uno sguardo al cammino compiuto dalla legge 12/2001 ad oggi. Rivista Italiana di Cure Palliative, 2009; 1.
17. *Nota: “La multidisciplinarità (o pluridisciplinarità) si realizza quando le competenze di discipline diverse vengono utilizzate in un’impresa conoscitiva o pratica comune, senza che ciascuna debba mutare le proprie prospettive concettuali o i propri metodi, ma limitandosi a fornire i propri “risultati”. In molti casi questo modo di procedere può essere sufficiente, ma non conduce ad una visione d’assieme in cui si veda come si rapportano i diversi aspetti studiati e come, eventualmente, si influenzino reciprocamente […] L’interdisciplinarità, infine, comporta la messa a confronto di ottiche diverse, lo sforzo di mutua integrazione fra queste, la consapevolezza della parzialità di ciascuna e nello stesso tempo della sua indispensabilità nella comprensione di un problema o di una realtà complessa […]. La vera interdisciplinarità […] si costruisce a partire dalle discipline e rispettando la serietà e l’impegno della loro tecnicità di indagine […] Non si può costruire l’interdisciplinarità se non sulla base di una solida competenza disciplinare”. Agazzi E. Cultura scientifica e interdisciplinarità. Brescia: Editrice La Scuola;1994:107-108; 111; 131.
18. Ministero della Salute, Il dolore cronico in medicina generale. 2010.
19. Cittadinanzattiva – Tribunale per i diritti del malato, Raccomandazione civica sul dolore cronico non oncologico. 2008.
20. Latina R, Graziano L, D’Angelo D, et al. La formazione accademica sul dolore in Italia: risultati di una indagine. In: Atti XVIII Congresso Nazionale Società Italiana di Cure Palliative (SICP) 2011. Trieste, 26-29 Ottobre 2011.
21. Robert Wood Johnson Foundation. A textbook case of nurses’ deficiency in pain management, end-of life care. Publications and Research. 2006.
22. Regione Piemonte, Azienda Sanitaria CN2 Alba-Bra, Lotta al dolore continuità assistenziale – ospedale e territorio. 2007.
23. Latina R, Mastroianni C, Ongari L, Zolli RM, Fabriani L, D’Angelo D, Casale G, Sansoni J, Di Biagio E, Tarsitani G and De Marinis MG. Conoscenze di base per la valutazione e gestione del dolore. Indagine sugli studenti italiani dei corsi di laurea sanitaria. Pain Nursing Magazine 2013; 2:13-19.
24.Sansoni J, Advanced Nursing Practice: some thoughts. Prof Inferm 2007;60(1):5-12.
25.Decreto 4 aprile 2012 – Istituzione del Master universitario di I livello in «Cure palliative evterapia del dolore» per professioni sanitarie. (12A04293) (GU n. 89 del 16-4-2012).
26. Master in Cure Palliative e terapia del dolore. Università Campus Bio-Medico, Roma, Available from:http://www.unicampus.it/offerta-formativa/master-i-livello-in-cure-palliative-e-terapia-del-dolore-per-le-professioni-sanitarie
27. American Association of Colleges of Nursing. (2005). DRAFT Essentials of the DNP. http://www.aacn.nche.edu/DNP/pdf/DNPEssentialsDraft_8-18-05.pdf.
28.De Marinis MG, Matarese M, et al. Un approccio didattico al problema del dolore nel diploma universitario per infermiere. Nursing oggi, 1999;3:1-7.
29.Lai YH, Chen ML, Tsai LY, et al. Are nurses prepared to manage cancer pain? A national survey of nurses’ knowledge about pain control in Taiwan. J Pain Sympt Manag, 2003;26:1016-1025.
Appendix
Pain management is the therapeutic process which focuses on the actions needed to intervene on what is the source of the pain, thus altering its perception and limiting its transmission to the central nervous system (1); as well, it is intended to improve the quality of life by searching for the most reliable methods used for the alleviation of pain and to allow a possible social and professional reintegration of the patient. This may be possible only if specific therapeutic approaches involving the psychological, spiritual, social, emotional and working life spheres are taken into account. The multidimensional nature of pain needs a global approach dealing with the different interventions which respond to the patients’ needs (2); as well, a multidisciplinary and interprofessional team is needed to gather all significant information on the patient and to record the outcome of the treatment, this latter essential to identify the best pain management plan.
Pain is a multidimensional and widespread phenomenon all over the world, but it is still a major issue which is under-evaluated and often inadequately treated (3). The undertreatment of pain, considered nowadays as a medical error (4), has several negative drawbacks on the health of people: it causes suffering, depression, loss of hope, reduction of the patient’s social functions, bad quality of life, absence from work. All this implies both a hospitalization rate which has doubled and a more frequent request for medical assistance: people suffering from chronic pain turn to emergency services five times more than those who do not suffer from chronic pain (5,6)